Piriformis Trigger Points | How To Find And Self Treat

Table of Contents
- - Piriformis Muscle Anatomy And Function
- - Piriformis Muscle vs. Sciatic Nerve — Why It Matters
- - What Are Trigger Points And Why Do They Matter?
- - Piriformis Trigger Point Locations
- - Main Complaints Related To Piriformis Trigger Points
- - Causes Of Piriformis Pain And Trigger Points
- - Deep Gluteal Pain Syndrome — The Bigger Picture
- - What Is Deep Gluteal Pain?
- - Causes Of Deep Gluteal Pain
- - Symptoms Of Deep Gluteal Pain
- - Deep Gluteal Pain vs. Other Conditions
- - Determining Piriformis And Deep Gluteal Pain
- - The Role Of MRI In Deep Gluteal Pain Syndrome
- - Top Tips For Dealing With Piriformis Pain
- - How To Self-Release Piriformis Trigger Points — 8 Techniques
- - Technique #1: Piriformis Relief Position
- - Technique #2: Piriformis Muscle Massage Therapy
- - Technique #3: Foam Roller Release
- - Technique #4: Tennis or Lacrosse Ball Release
- - Technique #5: Post-Isometric Relaxation (PIR)
- - Technique #6: Reciprocal Inhibition
- - Technique #7: Self-Massage With Foam Roll
- - Technique #8: The 90-90 Self-Release
- - Piriformis Stretches — 5 Techniques That Actually Work
- - Stretch #1: Supine Cross-Leg Glute Stretch
- - Stretch #2: Adduction and Hip Flexion Stretch
- - Stretch #3: Deep Piriformis Stretch With External Rotation
- - Stretch #4: 90-90 Piriformis Stretch (Floor)
- - Stretch #5: Standing 90-90 Piriformis Stretch
- - Follow-Up Exercises For The Piriformis
- - Exercises To Avoid With Piriformis Syndrome
- - Therapeutic Options — From Home Remedies To Surgery
- - When To Seek Professional Help
- - FAQs
- - How long does it take for piriformis pain to go away?
- - Can deep gluteal pain be chronic?
- - Should you stretch a sore piriformis?
- - What is the best way to prevent piriformis problems?
- - How does deep gluteal pain affect leg abduction?
- - When should I consider surgery?
- - Can deep gluteal pain be a sign of a more serious condition?
- - Are there risks associated with stretching the piriformis?
- - What are the long-term effects of piriformis pain?
Dealing with persistent hip or buttock pain? You might be experiencing the effects of piriformis trigger points. These sensitive spots within the piriformis muscle, located deep in the buttock region, can cause a wide range of symptoms — from localized discomfort to radiating pain that mimics sciatica.
Armed with my personal experience as a neuromuscular therapist with over 25 years of expertise and practical knowledge at my clinic Release Muscle Therapy, I’ll guide you through everything you need to know: how to identify, self-treat, and prevent piriformis trigger points, deep gluteal pain, and related conditions.
This is the most comprehensive resource you’ll find on this topic — covering anatomy, self-release techniques, stretching protocols, diagnostic imaging, and the full spectrum of treatment options.
Piriformis Muscle Anatomy And Function
Location: The piriformis muscle is located deep within the buttock, situated beneath the gluteal muscles.
Origin: It originates from the anterior surface of the sacrum, which is the triangular bone at the base of the spine.
Insertion: The muscle fibers run from the sacrum and converge to attach to the greater trochanter of the femur — the large bony prominence located on the outer side of the upper thigh.
Relation to the Sciatic Nerve: The piriformis is closely associated with the sciatic nerve, which either runs beneath or, in some individuals, through the muscle. This close proximity is the reason why the piriformis is often implicated in sciatic pain.
Key Functions Of The Piriformis Muscle
Lateral Rotation of the Hip: When the hip is extended, the piriformis acts primarily to laterally rotate the femur (thigh bone) in the hip joint. This means it helps turn the leg and foot outward.
Abduction of the Thigh: When the hip is flexed to 90 degrees, the piriformis acts to abduct the thigh, meaning it helps move the leg away from the midline of the body.
Stabilization: The piriformis also plays a role in stabilizing the hip joint, especially during walking or running. It helps keep the head of the femur securely within the hip socket, preventing dislocation or excessive movement.
Restraining Medial Rotation: The piriformis helps control and limit the medial (inward) rotation of the thigh, especially during the early stance phase of gait when the foot first hits the ground during walking.
Given its role and its relation to the sciatic nerve, any dysfunction or tightness in the piriformis can lead to a range of symptoms, the most notable being “piriformis syndrome.” This syndrome arises when the muscle compresses or irritates the sciatic nerve, leading to symptoms like buttock pain that can radiate down the leg, mimicking classic sciatica.
Piriformis Muscle vs. Sciatic Nerve — Why It Matters
The piriformis muscle plays an instrumental role in stabilization of the pelvis and hips. Due to its ability to assist in decelerating internal rotation of the femur, it should also be assessed in dysfunctional hips, knee pain, and also mechanical issues as far down as the foot.
Piriformis syndrome is a very common diagnosis which is often confused with sciatic pain. While some symptoms can overlap, sciatic nerve pain originates from the spine and is associated with numbness or tingling down the leg.
Piriformis pain tends to stay localized to the buttocks and is often directly made worse with aggressive stretching or exercises involving the glutes.
It is important to note that the concept of trigger points and their relationship to pain is a point of high debate in the clinical community. Regardless, it appears helpful to address these sensitive areas with trigger point release techniques, at least for temporary relief. Specifically, piriformis trigger point release can be attained by using simple neuromuscular techniques such as positional release technique, ischemic compression, or muscle energy techniques.

What Are Trigger Points And Why Do They Matter?
Trigger points, often referred to as “muscle knots,” are hypersensitive, tight areas or nodules within muscle fibers. They can be felt as small, tender lumps in the muscle and are usually the result of muscle overuse, strain, or injury.
There are two main types of trigger points:
Active Trigger Points: These cause pain at rest and when the muscle is used. The pain is usually felt at the site of the trigger point and can also radiate to other areas. This referred pain can sometimes follow specific patterns.
Latent Trigger Points: These are dormant and don’t cause spontaneous pain, but they can restrict movement and cause muscle weakness. When pressed or stretched, they can become painful.
Active trigger points are notorious for causing persistent pain, which can manifest as sharp, dull, burning, or aching sensations. This pain is sometimes so unique that it’s mistaken for other conditions, leading to potential misdiagnosis.
They can significantly impact the range of motion in joints due to the pain and muscle tightness they induce. Over prolonged periods, this limitation can escalate into joint stiffness and a noticeable decline in functionality.
Moreover, muscles plagued with active trigger points don’t operate at their best, resulting in muscle weakness and quick fatigue. One of the hallmark features of trigger points is their capability to refer pain to distant regions of the body — for example, those present in the neck might be the culprits behind recurring headaches.
Chronic presence of these trigger points, especially in pivotal muscles like those in the back and neck, can lead to postural anomalies as the body constantly tries to adjust and compensate for the pain and imbalance. The consistent pain and discomfort can also be a significant disruptor of sleep, causing conditions like insomnia or sporadic sleep patterns.
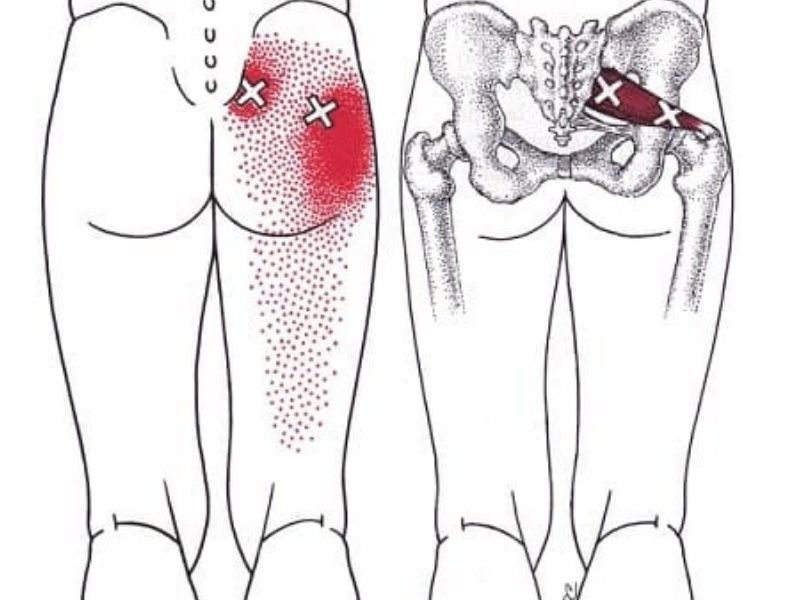
Piriformis Trigger Point Locations
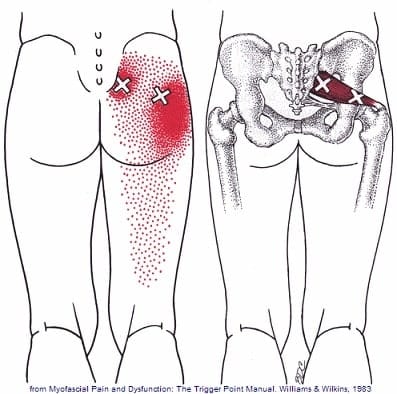
Image reference: David G. Simons, Janet G. Travell, Lois S. Simons. Myofascial Pain and Dysfunction: The Trigger Point Manual
The piriformis muscle, given its relatively small size but significant depth, can house multiple trigger points. The exact number and precise location can vary among individuals, but typically, the trigger points in the piriformis muscle are found in the following areas:
Medial Trigger Point: Located closer to the sacrum, this trigger point is found near the muscle’s origin on the anterior surface of the sacrum. It’s often the most medial of the piriformis trigger points.
Central Trigger Point: Positioned roughly in the middle of the muscle belly, this trigger point is typically the most prominent and can be the primary source of referred pain patterns associated with the piriformis.
Lateral Trigger Point: Located closer to the greater trochanter of the femur where the piriformis inserts, this trigger point is the most lateral and can sometimes be the source of pain that radiates down the leg.
When palpating (feeling) for these trigger points, one might feel taut bands or nodules within the muscle, which are hypersensitive to pressure. Applying pressure to these points can reproduce the pain or refer pain to other areas, a characteristic feature of trigger points.
It’s essential to approach piriformis trigger points with care, given the muscle’s proximity to the sciatic nerve. Proper assessment and treatment by trained professionals can ensure that the nerve is not inadvertently irritated during the process.
Main Complaints Related To Piriformis Trigger Points
Trigger points in the piriformis muscle can lead to a variety of symptoms and complaints. Due to its proximity to the sciatic nerve, the piriformis can have a profound impact when these trigger points become active:
Buttock Pain: One of the most common complaints is a deep, aching pain in the buttock on the affected side. This pain can sometimes be sharp or radiating.
Sciatica-like Symptoms: The sciatic nerve runs very close to or even through the piriformis muscle in some individuals. When the piriformis muscle becomes tight or inflamed due to trigger points, it can compress or irritate the sciatic nerve, leading to symptoms that mimic sciatica — radiating pain, tingling, or numbness that travels down the leg, sometimes reaching as far as the foot.
Reduced Range of Hip Motion: The tightness and discomfort caused by the trigger points can lead to a reduction in the range of motion of the hip joint, making movements like hip rotation painful.
Referred Pain: Trigger points in the piriformis can also cause referred pain to other areas, such as the lower back or the other regions of the buttock.
Difficulty Sitting: Due to the location of the piriformis, sitting for extended periods, especially on hard surfaces, can exacerbate the pain and discomfort.
Pain While Walking: Walking, especially for long distances, can become painful due to the involvement of the piriformis in hip stabilization and movement.
Pain During Certain Activities: Activities that put strain on the piriformis, such as climbing stairs, running, or even crossing legs, can become painful when there are active trigger points in the muscle.
Signs You May Have Piriformis Issues
- Lower back pain
- Sacroiliac joint pain
- Sciatica-type symptoms
- Hip pain
- Posterior pelvic tilt
- Pelvic pain
- Difficulty lying on your back with legs straight
- Sciatic-type sensations after sitting too long
Causes Of Piriformis Pain And Trigger Points
Piriformis pain and the development of trigger points in the muscle can arise from various causes:
Muscle Overuse or Strain — Often seen in athletes or individuals who engage in activities requiring repetitive hip rotation or sudden changes in direction.
Direct Trauma — Injury to the buttock area, such as from a fall or a car accident, can lead to inflammation and tightness in the piriformis, fostering the formation of trigger points.
Prolonged Sitting — Especially on hard or uneven surfaces, constant pressure on the muscle leads to discomfort and potential trigger point development.
Anatomical Variations — In some individuals, the sciatic nerve runs through the piriformis muscle rather than beneath it (approximately 16–17% of the population), making them more susceptible to piriformis syndrome.
Postural and Gait Imbalances — Issues in adjacent muscles or joints can place undue stress on the piriformis, contributing to pain and the onset of trigger points.
Asymmetry and Dominance Patterns — Asymmetry is normal in the human body, and we tend to be more right-side dominant when it comes to weight bearing. On a weight-bearing side, the hip is positioned into internal rotation. The opposite hip is in a relatively externally rotated position. This means the piriformis is at a slightly different length on each side, and stretching or strengthening may need a different approach depending on the symptomatic side.
Other Conditions — Lumbar spine issues or hip disorders can refer pain to the piriformis region, making it essential to obtain a comprehensive diagnosis to pinpoint the exact cause of the discomfort.
Deep Gluteal Pain Syndrome — The Bigger Picture
Piriformis trigger points don’t exist in a vacuum. They’re part of a larger clinical picture known as Deep Gluteal Pain Syndrome (DGPS) — a relatively new umbrella term that encompasses all conditions causing sciatic nerve entrapment in the deep gluteal space.
What Is Deep Gluteal Pain?
It’s a sensation of numbness or distinct pain in the buttocks that often causes radiating pain along the sciatic nerve distribution. Unlike regular buttock pain, deep gluteal pain is considered a sciatic nerve disorder. It is untethered from disc issues and features sciatic nerve entrapment in the deep gluteal space.
Deep gluteal pain is not a minor inconvenience. It can become a disabling problem in older adults and a performance killer in young people.
Causes Of Deep Gluteal Pain
The deep gluteal space is complex, and each component can be a pain trigger:
Entrapment Neuropathy — Pinching or pressure upon a nerve, which triggers pain. The piriformis muscle is one of the most common culprits.
Lesions and Fractures — Inflammation originating from an injury or fracture. Repetitive movements can cause micro-tears in the muscle tissue that swell and put pressure on nerve structures.
Enthesopathy and Tendinopathy — Tendon disorders such as tendinitis can cause deep gluteal pain. Potential culprits include the quadratus femoris muscle, piriformis muscle, and gluteus medius.
Uncommon Causes — Some patients develop deep gluteal pain during pregnancy or ovulation due to referred pain from intra-abdominal or intra-pelvic inflammatory processes. Endometriosis, irritable bowel syndrome, and even inguinal hernia may cause these symptoms. Trigger points in the gluteals may also be a contributing factor.
Symptoms Of Deep Gluteal Pain
- Buttock pain or numbness
- Pain radiated to the knee (sciatic nerve symptoms)
- Pain triggered by prolonged sitting
- Walking in short strides for pain avoidance
- Sensory changes and pain upon palpation
- Disturbed sleep due to severe pain at night
- Locking or clicking sounds on the hip joint
- Limping after prolonged sitting
These symptoms do not follow a set script. Nerve entrapment can be vague and hard to pinpoint. Symptoms may come and go and change location, varying in intensity depending on the cause.
Specific conditions may present differently. For example, hamstring tendinopathy could make you feel a “boggy mass” in your hips with weight-bearing activities. Gluteal tendinopathy gives you night pain when lying on the affected side. In pudendal nerve entrapment, using a seat or riding a bicycle increases the pain, but sitting on a toilet might bring some relief.
Deep Gluteal Pain vs. Other Conditions
Piriformis Syndrome — The term has been around since the 1930s. Today, deep gluteal syndrome casts a wider net, encompassing piriformis syndrome plus new entities health professionals should consider.
Proximal Hamstring Tendinopathy — Occurs due to repetitive loading and strain. Repetitive motion causes micro-tears, inflammation, thickening of the tendon, and compression of the sciatic nerve.
Trochanteric Bursitis — Features inflammation in the bursa of the greater femoral trochanter. People typically present with pain on the outside of the hip and posterior thigh.
Determining Piriformis And Deep Gluteal Pain
Physical Examination
Physical therapists may assess whether hip flexion or rotation worsens the pain and whether it flares up during physical activity or extended sitting. Through physical examination, paresthesia, numbness, trigger points, and tender areas can be detected. Different landmarks guide palpation, including the greater trochanter, ischial tuberosity, and iliac crest.
Special Tests
Special tests include internal rotation of the hip, the flexion test, and the seated piriformis stretch test. The piriformis muscle provocation test is also beneficial to diagnose sciatic nerve entrapment.
Diagnostic Imaging
X-rays can spot bone pathologies. Nerve conduction studies help detect sciatic nerve entrapment. However, an MRI is the most convenient to rule out specific underlying contributors and assist with diagnosing the root cause. Ultrasound can also play a crucial role, adding real-time evaluations while guiding palpation and identifying structures likely to be a source of pain.
The Role Of MRI In Deep Gluteal Pain Syndrome
MRI is the most commonly used tool by physicians to investigate deep gluteal syndrome anatomy. But like other diagnostic tools, it has limitations.
MRI Accuracy
Research pooling 239 cases of sciatica of non-disc origin revealed a specificity of 93% and a sensitivity of 64%. This means false positives are very uncommon, but there is a high incidence of false negatives. Many patients could have deep gluteal syndrome anatomy issues even if they don’t show up on their MRI. An MRI should confirm the diagnosis or rule out other causes — it is not a screening test.
How MRI Findings Affect Treatment
Depending on the MRI findings, the therapy plan takes shape:
Piriformis Syndrome — MRI may show hypertrophy and anatomical variants of the piriformis muscle. Treatment usually consists of anti-inflammatory medications, muscle relaxants, rest, and a 6-week course of exercises. If conservative approaches fail, botulinum toxin injection and surgical resection may be considered.
Sciatic Nerve Variants — Around 16–17% of the population has an abnormal course of the sciatic nerve inside the deep gluteal space. If conservative treatment fails, an endoscopic tenotomy of the piriformis muscle is the treatment of choice.
Piriformis Muscle Variants — An anatomical variant can alter the interaction between the piriformis muscle and the sciatic nerve. These cases are usually more difficult to resolve and may require endoscopic muscle resection.
Trauma and Overuse — MRI can detect fibrous bands that form in response to inflammation. The most effective treatment is often endoscopic sciatic nerve decompression.
Hamstring Tendinopathy — Images may feature acute inflammation and edema affecting the sciatic nerve, or chronic fibrotic tissue. Many acute cases respond to conservative treatment; chronic cases may require surgery.
Limitations Of MRI
MRI has key limitations to understand:
Dynamic Entrapment — A type of piriformis syndrome involves sciatic nerve entrapment that only occurs during certain postures or movements. MRI cannot capture this.
Orthopedic Anomalies — When sciatic pain is triggered by orthopedic issues, these are not always visible on MRI because the neuropathy is activated only during dynamic motion.
All diagnostic tools should guide and not replace clinical tests. A postural evaluation, gait examination, and physical exam maneuvers can lead the diagnostic suspicion to a more accurate location.
Top Tips For Dealing With Piriformis Pain
Before jumping into release techniques, consider these practical tips:
- Avoid crossing your legs and generally sitting with your knees too close together
- Avoid excessive aggressive stretching of the piriformis — this often makes things worse
- Avoid intense strength training that fatigues already painful and sensitive tissues
- Emphasize placing the affected-side leg into external rotation to allow the muscle to passively shorten and relax
- Use a cane or walking sticks temporarily if it’s painful to walk
- Use passive therapies such as heat or ice, pain relief creams, or TENS to calm down nerves and promote circulation
- Strengthen the other gluteal muscles and reduce over-activity of antagonist muscles
The Piriformis Relief Position
When piriformis pain is just too aggravated and sensitive to stretch or exercise, sometimes the best thing to do is simply get into a position of relief.
Lay face down and place the affected leg out to the side. This position allows the piriformis muscle to shorten, which can help relieve tension and allow it to calm down. A small pillow can be placed under the hip to reduce lower back discomfort. Usually 3–5 minutes is sufficient to allow a reduction in excess muscle tone, but it can be done for much longer if desired.
How To Self-Release Piriformis Trigger Points — 8 Techniques
Technique #1: Piriformis Relief Position
(Described above) — When pain is too aggravated for any active work, start here.
Technique #2: Piriformis Muscle Massage Therapy
The piriformis muscle lies under the larger, more superficial glute muscles, so it can be challenging to directly reach until those layers are relaxed. This muscle is responsive to gentle approaches and does not need overly aggressive pressure to get results. Even simple glides with thumbs or the elbow are effective.
The fibers connect to the anterior (front) surface of the sacrum bone, so they can be challenging to fully address — which is why a combination of deep tissue massage and stretching work is often indicated for best results.
Caution for Piriformis Syndrome: Since the muscle is already aggravated, excessive intensity can further increase sensitivity, pain, and guarding. A gentle, graded exposure approach is essential. Since the intensity is generally low, it may be necessary to follow up with exercises and stretches to get the release to “stick.”
Technique #3: Foam Roller Release
Sit on a foam roller and position it under the buttock of the affected side. Gently roll back and forth, applying sustained pressure on tender areas to help release muscle tightness. The foam roller provides a soft surface, and the wider contact area makes it the most tolerable tool to start with.
Technique #4: Tennis or Lacrosse Ball Release
Place a tennis or lacrosse ball under the buttock and lean into it. Target specific trigger points more precisely, applying pressure and making small circular movements. Note: using a softball or lacrosse ball can be quite uncomfortable due to the concentrated pressure per square inch. This may result in an inability to relax fully, trigger guarding, and reduce effectiveness — especially important when dealing with piriformis syndrome.
Technique #5: Post-Isometric Relaxation (PIR)
Post-isometric relaxation works very well for the hip muscles. Contract the piriformis at a low intensity for 8–10 seconds, then fully relax into the new stretch position for another 8–10 seconds. Repeat several times.
Technique #6: Reciprocal Inhibition
This is a very powerful release technique for the piriformis and other external hip rotators because the groin (especially on the left side) is often inhibited and needs to be strengthened. By actively engaging the opposing muscle group, the piriformis reflexively relaxes.
Technique #7: Self-Massage With Foam Roll
You can perform self myofascial release by foam rolling the piriformis, using a lacrosse ball, or a softball. Start with the foam roller for gentlest contact, then progress as tolerated.
Technique #8: The 90-90 Self-Release
The 90-90 stretch is an excellent self piriformis release that combines stretch with gentle pressure in a seated position.
Piriformis Stretches — 5 Techniques That Actually Work
Stretching the piriformis after trigger point release is vital. The process ensures the muscle retains its relaxed state, prevents re-tightening, boosts blood flow, and speeds up recovery. A flexible piriformis functions more efficiently and reduces potential injuries.
Important: Make sure you have warmed up before stretching. An easy way to warm up is a few minutes of light aerobic exercise like walking — this is often the easiest and fastest way to reduce subconscious tension and guarding.
Stretch #1: Supine Cross-Leg Glute Stretch
Lie on your back with legs straight. Bend one leg and place the foot just outside the opposite knee. Use your opposite hand and gently pull the knee across the body and up slightly toward the hip. You will feel a stretch on the outside of the hip. Hold for 30 seconds, repeat 2–3 times.
This is often the most comfortable stretch to start with.
Stretch #2: Adduction and Hip Flexion Stretch
Because of the piriformis location and hip mechanics, there are two different approaches to stretching it. In this version, the emphasis is on adduction and hip flexion, which allows for release of the more superficial muscles and some of the external hip rotators.
Stretch #3: Deep Piriformis Stretch With External Rotation
This second variation can directly target the piriformis and is generally performed AFTER the adduction stretch. A combination of varying hip positions with external rotation will get most of the deep hip muscles stretched.
Stretch #4: 90-90 Piriformis Stretch (Floor)
Sit on the floor with one leg out in front of you at a 90-degree angle from your body. The other leg should be placed to the side with the knee at a 90-degree bend. While maintaining the arch (lordosis) of the lower spine, tip your pelvis forward as though it were a bucket of water. You should feel a stretch in the gluteal area. Hold for 30 seconds, repeat 2–3 times.
Stretch #5: Standing 90-90 Piriformis Stretch
This standing version is virtually identical to the floor version. It is most helpful when it’s not possible to get down on the floor, or if there isn’t enough hip mobility for the floor version. Place the bent leg on a table, keep the opposite knee bent for balance, and from the starting position, tip your hips forward until you feel the stretch. Hold for 30 seconds, repeat 2–3 times.
Follow-Up Exercises For The Piriformis
Post-trigger point release, follow-up exercises are paramount to ensure sustained muscle health and functionality. While release targets immediate tension, exercises reinforce muscle strength, endurance, and coordination.
By actively engaging the piriformis and its neighboring muscles, these exercises foster muscle memory, ensuring the piriformis operates in harmony with surrounding structures. This reduces the risk of muscle imbalances (a precursor to injuries and strain) and supports optimal hip and pelvic mechanics during daily activities.
Consistent exercises act as a preventive measure, deterring the re-emergence of trigger points by keeping the muscle active and well-circulated. While trigger point release provides immediate relief, follow-up exercises lay the foundation for long-term piriformis health and optimal biomechanical function.
Exercises To Avoid With Piriformis Syndrome
If you have active piriformis syndrome, certain exercises can make things worse:
Sidelying Clamshells — Often assigned early in rehab, but they tend to be too much of a “direct hit” on the muscle. Since it’s hard to perform them with low-enough intensity, it’s best to hold off until the muscle is less irritated and pain has been reduced.
Lateral Band Walks — Avoid for the same reason as clamshells — they are usually not well-tolerated when the piriformis is aggravated.
Pay attention to how your body feels during each exercise and don’t push too hard. Go slowly, focus on proper form, allow time to rest between sets, and always listen to what your body is telling you.
Therapeutic Options — From Home Remedies To Surgery
Home Therapy
Activity Modifications — Depending on the source of pain, changes may be needed. For hamstring tendinopathy, avoid bending activities, especially deadlifts, and avoid stretching the hamstrings unless directly recommended by your therapist. Alternate periods of sitting and standing. Drivers should move the seat closer to the steering wheel. Runners may need to reduce stride length.
Additional Home Recommendations — Shed excess weight and quit smoking if applicable. Anti-inflammatory foods can be helpful, such as turmeric and omega-3. Ice can improve pain temporarily — use a cloth to keep skin apart, and limit ice therapy to five minutes to avoid ice burns.
Self-Massage — You can benefit from self-massage at home with foam rollers or a tennis ball (see the 8 techniques above).
Professional Therapy
Medications — Oral analgesics are often the first-line treatment. Muscle relaxants may be added when the source is muscle tension. More severe cases may require intramuscular or intravenous therapy.
Physical Therapy — Most professionals recommend rehabilitation for a minimum of six weeks, consisting of exercises to strengthen hip mechanics, tendons, and muscles involved in lower extremity movement. Some exercises are designed to mobilize sciatic nerve entrapment through nerve gliding techniques.
Massage Therapy — Neuromuscular massage therapy, also referred to as myofascial release or trigger point therapy, consists of applying pressure for 30 seconds to two minutes with appropriate intensity on the correct trigger point. This technique should be administered by a professional for best results.
Experimental and Complementary Treatment — Some cases improve with trigger point injections and acupuncture. There are reports showing results with botulism toxin injections in the piriformis muscle, though this approach can cause complications such as fibrosis of the sciatic nerve.
Surgical Treatment — Sometimes surgery is the only resource to achieve pain relief. Options include open decompression of the sciatic nerve or endoscopic procedures. For severe cases, this can be a game-changer in hamstring or piriformis muscle syndrome and traumatic causes of deep gluteal syndrome.
When To Seek Professional Help
If your pain persists after trying self-care measures such as rest and stretching, seek professional advice from a physical therapist before attempting further activity that could exacerbate your symptoms.
When dealing with issues like piriformis syndrome, proper assessment for underlying causes (such as lumbar pathology) and personalized care are essential for successful recovery. Remember: other problems outside the deep gluteal space — such as hip joint osteoarthritis or femoral neck fractures — can also trigger these symptoms.
Do not hesitate to come to a professional for deep gluteal pain. Most patients find relief through conservative treatment and physical therapy, making a profound difference in their quality of life.
FAQs
How long does it take for piriformis pain to go away?
With consistent stretching and gentle exercises, most simple cases of piriformis pain improve within a few weeks. Recovery from deep gluteal pain may take 6 to 12 weeks, depending on the trigger and severity. During this time, follow the instructions of your doctor or therapist to speed up results.
Can deep gluteal pain be chronic?
Yes. Chronic deep gluteal pain can develop when a long-standing ailment is causing symptoms. Some cases of recurrent or refractory pain can reach a chronic state. Supportive therapy rather than a curative approach may be needed.
Should you stretch a sore piriformis?
If you have a mild case of muscle spasms or strain, a gentle stretch may help. In cases of severe inflammation or nerve irritation, a more specialized approach is needed. If pain persists, seek professional advice before continuing.
What is the best way to prevent piriformis problems?
Regular stretching, strengthening exercises (especially the other gluteal muscles), and staying active throughout the week with activities such as walking or cycling. Avoid prolonged sitting, and pay attention to posture and gait.
How does deep gluteal pain affect leg abduction?
Deep gluteal pain with leg abduction can be a sign of piriformis muscle involvement. This movement may be used during physical examination to identify the source of pain.
When should I consider surgery?
Surgery is the last treatment option for patients who do not respond to medical treatment and physical therapy. In most cases, conservative treatment is sufficient.
Can deep gluteal pain be a sign of a more serious condition?
Yes. Hip joint osteoarthritis, femoral neck fractures, and other serious injuries outside the deep gluteal region can trigger similar symptoms. A thorough evaluation is essential.
Are there risks associated with stretching the piriformis?
Incorrect form could lead to further irritation. If your condition has progressed beyond basic muscular tension, stretching may not provide much benefit. Always listen to your body and take appropriate measures.
What are the long-term effects of piriformis pain?
If left untreated, the piriformis remaining in an overly contracted state could lead to other areas of tension, joint instability, additional pains, and may affect your ability to move freely through everyday activities.
References:
- Podschun, L., Hanney, W. J., Kolber, M. J., Garcia, A., & Rothschild, C. E. (2013). Differential diagnosis of deep gluteal pain in a female runner with pelvic involvement: a case report. International Journal of Sports Physical Therapy, 8(4), 462.
- Hu, Y. W. E., Ho, G. W., & Tortland, P. D. (2021). Deep gluteal syndrome: a pain in the buttock. Current Sports Medicine Reports, 20(6), 279-285.
- McCrory, P., & Bell, S. (1999). Nerve entrapment syndromes as a cause of pain in the hip, groin, and buttock. Sports Medicine, 27, 261-274.
- Franklyn-Miller, A., Falvey, E., & McCrory, P. (2009). The gluteal triangle: a clinical patho-anatomical approach to the diagnosis of gluteal pain in athletes. British Journal of Sports Medicine, 43(6), 460-466.
- Ohm-Pedersen, K. (2018). Gluteal Tendinopathy. Clinical Practice Guidelines, 357.
- Carro, L. P., et al. (2016). Deep gluteal space problems: piriformis syndrome, ischiofemoral impingement, and sciatic nerve release. Muscles, Ligaments and Tendons Journal, 6(3), 384.
- Martin, H. D., & Gómez-Hoyos, J. (2019). Deep gluteal syndrome. Posterior Hip Disorders: Clinical Evaluation and Management, 167-187.
- Hernando, M. F., et al. (2015). Deep gluteal syndrome: anatomy, imaging, and management of sciatic nerve entrapments in the subgluteal space. Skeletal Radiology, 44(7), 919-934.
- Chang, K. V., et al. (2018). Ultrasound imaging and guided injection for the lateral and posterior hip. American Journal of Physical Medicine & Rehabilitation, 97(4), 285-291.
- Awan, W. A., & Babur, M. N. (2011). Effectiveness of deep friction massage & stretching exercises in piriformis syndrome. IJCRB, 3(03), 378-383.

Sam Visnic
I’ve spent my life studying the fundamental aspects of human health with a focus on movement and clinical massage therapy. In a world of specialists, surgical procedures, drugs and quick fix remedies, I’m committed to finding and developing strategies that help people stuck at the “gap”. Over the last 20 years I’ve studied dozens of systems and methodologies for uncovering the root cause of aches and pains, along with postural and movement issues. Pain science, the art and science of hands-on soft tissue massage techniques, myofascial release, and coaching movement is essential in my practice. Integrating different methods but above all deciphering WHEN to use different techniques with different people and situations, along with integration of movements that people want to be able to do again is the key to long term success with my incredible track record with clients. Understanding the various elements that contribute to conditions and the power of communication and education makes my Release Muscle Therapy program separate from other hands-on therapy approaches.












